Education
Case Report: Application of Frameless Stereotaxy to Brain Tumor Surgery
A 16-year-old female presented with new onset seizures that resolved following initiation of anticonvulsant therapy.
Brain imaging studies showed a heterogeneously-enhancing posterior right temporal mass with multiple cysts (Figures 1 and 2).
 Figure 1 - T1 weighted coronal image following contrast administration shows a multicystic mass with heterogeneous enhancement in the right posterior temporal lobe. Thickening and pneumatization of the lateral temporal bone in relation to the lower half of the mass are well demonstrated on this image.
Figure 1 - T1 weighted coronal image following contrast administration shows a multicystic mass with heterogeneous enhancement in the right posterior temporal lobe. Thickening and pneumatization of the lateral temporal bone in relation to the lower half of the mass are well demonstrated on this image.
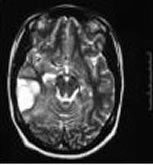 Figure 2 - T2 weighted axial image showing multiple cysts and distortion of the adjacent brain parenchyma.
Figure 2 - T2 weighted axial image showing multiple cysts and distortion of the adjacent brain parenchyma.
For posterior temporal masses, frameless stereotaxy using a neuronavigational system based on MRI fiducials is useful in accurately executing the surgical plan by allowing:
- Identification of the margins of the surface and subcortical contours of the mass;
- Identification of the extent and position of thickening/pneumatization of the lateral temporal bone;
- Identification of the junction of the transverse and sigmoid sinuses;
- Identification of the position of the vein of Labbe and other bridging veins.
For this case, the surgical plan required accurate positioning of a craniotomy flap centered on the mass yet respecting the extensive thickening/pneumatization of the lateral temporal bone. In reviewing the coronal images, the position of the inferior craniotome cut would be difficult to determine precisely based only on external landmarks.
Frameless stereotaxy using the neuronavigational system (Stryker, Kalamazoo, MI) was used to mark out the margins of the craniotomy and the position of the inferior craniotome cut. The remaining bone removal was performed as a subtemporal craniectomy by drilling out the thickened/pneumatized portion of the lateral temporal bone to bring the exposure closer to the floor of the middle cranial fossa. This allowed better visualization of the posterolateral bridging veins, thus preventing inadvertent avulsion and uncontrolled hemorrhage.
 Figure 3 - In this operative display, the coronal image (upper left corner) shows the caudalmost level at which the craniotome may be safely used to turn out the bone flap based on the extent of thickening/pneumatization of the lateral temporal bone. The position of the transverse sinus coursing towards its junction with the sigmoid sinus is well demonstrated on the axial view (lower left corner).
Figure 3 - In this operative display, the coronal image (upper left corner) shows the caudalmost level at which the craniotome may be safely used to turn out the bone flap based on the extent of thickening/pneumatization of the lateral temporal bone. The position of the transverse sinus coursing towards its junction with the sigmoid sinus is well demonstrated on the axial view (lower left corner).
 Figure 4 - The neuronavigational pointer is shown corresponding to the images in Figure 3. Dots mark the relative margins of the mass posteriorly, superiorly (bottom of figure), and anteriorly. The transverse line represents the level at which the craniotome may be brought across the flap without abutting the thickened/pneumatized temporal bone.
Figure 4 - The neuronavigational pointer is shown corresponding to the images in Figure 3. Dots mark the relative margins of the mass posteriorly, superiorly (bottom of figure), and anteriorly. The transverse line represents the level at which the craniotome may be brought across the flap without abutting the thickened/pneumatized temporal bone.